Ulcerative Colitis
What is ulcerative colitis?
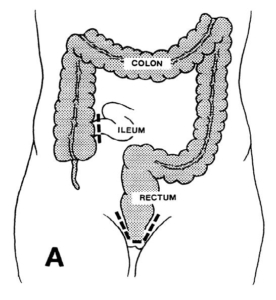
Ulcerative colitis is an inflammation of the lining of the large bowel (colon and rectum). Symptoms include rectal bleeding, diarrhea, abdominal cramps, weight loss, and fevers. In addition, patients who have had extensive ulcerative colitis for many years are at an increased risk to develop large bowel cancer. The cause of ulcerative colitis remains unknown.
How is ulcerative colitis treated?
Initial treatment of ulcerative colitis is medical, using antibiotics and anti-inflammatory medications such as aminosalicylates. If these fail, prednisone can be used for a short period of time but long-term use can be associated with significant side effects. If prednisone is ineffective or cannot be discontinued, immunomodulators such as 6-mercaptopurine or azathioprine can be used to control active disease that does not merit hospitalization. In order to maintain control of the disease, aminosalicylates or immunomodulators are used on a long-term basis. “Flare-ups” of the disease can often be treated by increasing the dosage of medications or adding new medications. Hospitalization may be necessary to put the bowel to rest and deliver steriods directly into the blood stream.
When is surgery necessary?
Surgery is indicated for patients who have life-threatening complications of inflammatory bowel diseases, such as massive bleeding, perforation, or infection. It may also be necessary for those who have the chronic form of the disease, which fails to improve with medical therapy. It is important the patient be comfortable that all reasonable medical therapy has been attempted prior to considering surgical therapy. In addition, patients who have long-standing ulcerative colitis may be candidates for removal of the large bowel, because of the increased risk of developing cancer. More often, these patients are followed carefully with repeated colonoscopy and biopsy, and surgery is recommended only if precancerous signs are identified.
What operations are available?
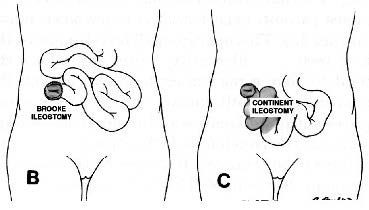
Historically, the standard operation for ulcerative colitis has been removal of the entire colon, rectum, and anus. This operation is called a proctocolectomy (Illustration A) and may be performed in one or more stages. It eliminates the disease and removes all risk of developing cancer in the colon or rectum. However, this operation requires creation of a Brooke ileostomy (bringing the end of the remaining bowel through the abdomen wall, Illustration B) and long-term use of an appliance on the abdominal wall to collect waste from the bowel.
The continent ileostomy ( Illustration C) is similar to a Brooke ileostomy, but an internal reservoir is created. The bowel still comes through the abdominal wall, but an external appliance is not required. Instead, the internal reservoir is drained three to four times a day by inserting a tube into the reservoir. This option eliminates the risks of cancer and risks of recurrent persistent colitis, but the internal reservoir may begin to leak and require another surgical procedure to revise the reservoir.
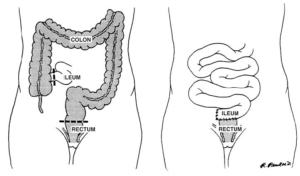
Some patients may be treated by removal of the colon, with preservation of the rectum and anus. The small bowel can then be reconnected to the rectum and continence preserved. This avoids an ileostomy, but the risks of ongoing active colitis, increased stool frequency, urgency, and cancer in the retained rectum remain.
Are there other surgical alternatives?
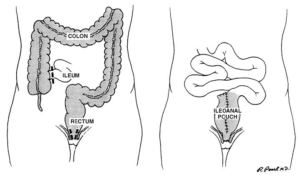
The ileoanal procedure is the most common surgical treatment for the management of ulcerative colitis. This procedure removes all of the colon and rectum, but preserves the anal canal. The rectum is replaced with small bowel, which is refashioned to form a small pouch. Usually, a temporary ileostomy is created, but this is closed several months later. The pouch acts as a reservoir to help decrease the stool frequency. This maintains a normal route of defecation, but most patients experience five to ten bowel movements per day. This operation all but eliminates the risk of recurrent ulcerative colitis and allows the patient to have a normal route of evacuation. Patients can develop inflammation of the pouch (pouchitis), which usually responds to antibiotic treatment. In a small percentage of patients, the pouch fails to function properly and may have to be removed. If the pouch is removed, a permanent ileostomy will likely be necessary.
Which alternative is preferred?
It is important to recognize that none of these alternatives makes a patient with ulcerative colitis normal. Each alternative has perceivable advantages and disadvantages, which must be carefully understood by the patient prior to selecting the alternative which will allow the patient to pursue the highest quality of life.