Practice Parameters for Sigmoid Diverticulitis
Janice Rafferty, M.D., Paul Shellito, M.D., Neil H. Hyman, M.D., W. Donald Buie, M.D., and the Standards Committee of The American Society of Colon and Rectal Surgeons
The American Society of Colon and Rectal Sur-geons is dedicated to assuring high-quality patient care by advancing the science, prevention, and management of disorders and diseases of the colon, rectum, and anus. The Standards Committee is com-posed of Society members who are chosen because they have demonstrated expertise in the specialty of colon and rectal surgery. This Committee was created to lead international efforts in defining quality care for conditions related to the colon, rectum, and anus. This is accompanied by developing Clinical Practice Guidelines based on the best available evidence. These guidelines are inclusive, and not prescriptive. Their purpose is to provide information on which decisions can be made, rather than dictate a specific form of treatment. These guidelines are intended for the use of all practitioners, health care workers, and patients who desire information about the manage-ment of the conditions addressed by the topics covered in these guidelines. It should be recognized that these guidelines should not be deemed inclusive of all proper methods of care or exclusive of meth-ods of care reasonably directed to obtaining the same results. The ultimate judgment regarding the propri-ety of any specific procedure must be made by the physician in light of all of the circumstances pre-sented by the individual patient.
PRACTICE GUIDELINE: SIGMOID DIVERTICULITIS
These guidelines address the evaluation and man-agement of sigmoid diverticulitis and are built on the last set of guidelines for the treatment of diverticulitis published by The American Society of Colon and Rectal Surgeons (ASCRS) in 2000.1 Additional perti-nent information from the published literature from January 2000 to August 2005 was retrieved and re-viewed. Searches of MEDLINE were performed by using keywords: diverticulitis, diverticulosis, peridiverticulitis, and fistula.
STATEMENT OF PROBLEM
Acquired colonic diverticular disease affects the sigmoid colon in 95 percent of cases. Thirty-five per-cent of patients with sigmoid diverticulosis also have disease in the more proximal colon. Diverticula are rare below the pelvic peritoneal reflection. Prevalence correlates with age; approximately 30 percent of the population has acquired diverticular change by age 60 years, whereas almost 60 percent of those aged 80 years and older are affected. Ten to 25 percent of patients with diverticulosis will develop diverticulitis.2–12
Initial Evaluation of Acute Diverticulitis
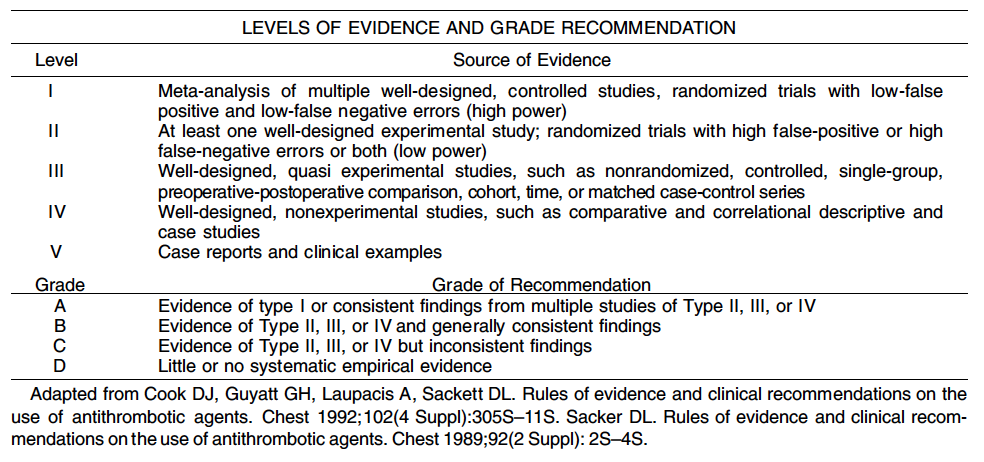
1. The initial evaluation of a new patient with suspected acute diverticulitis should include a problem-specific history and physical examination; a complete blood count (CBC), urinalysis, and plain abdominal radiographs may be useful in selected clinical scenarios. Level of Evidence: V; Grade of Recommendation: D.
A diagnosis of acute diverticulitis often can be made based on history and physical findings, especially in patients who have had previously confirmed diverticulitis. However, in many cases of abdominal pain, it may be uncertain whether acute diverticulitis is present and adjunctive studies are helpful and warranted. Alternative diagnoses include irritable bowel syndrome, gastroenteritis, bowel obstruction, inflammatory bowel disease, appendicitis, ischemic colitis, colorectal cancer, urinary tract infection, kidney stone, and gynecologic disorders. An elevated white blood cell count often is helpful in confirming the presence of an inflammatory process. Pyuria may reveal a urinary tract infection, and hematuria may suggest a kidney stone. Plain abdominal films may show pneumoperitoneum from a perforated viscus, or signs of bowel obstruction.
2. Computerized tomography (CT) scan of the abdomen and pelvis is usually the most appropriate imaging modality in the assessment of suspected diverticulitis. Level of Evidence: III; Grade of Recommendation: A.
CT scan is typically the examination of choice for patients with suspected diverticulitis who require diagnostic imaging. Accuracy is enhanced if oral, intravenous, and rectal contrast are used. It is highly sensitive and specific, with a low false-positive rate.13 Complications, such as phlegmon, abscess, adjacent organ involvement, fistula, and distant septic complications, can be identified. The positive predictive value for diverticulitis by CT scan is 73 percent for the presence of sigmoid diverticula, 88 percent for pericolic inflammation, 85 percent for wall thickness of 7 to 10 mm, and 100 percent for wall thickness >10mm. A large abscess found on initial CT scan may prompt early percutaneous drainage and, consequently, shorten the hospitalization. Severity staging by CT scan may allow selection of patients most likely to respond to conservative therapy.15–17 The severity of diverticulitis at the time of the first CT scan not only predicts an increased risk of failure of medical therapy on index admission but also a high risk of secondary complications after initial nonoperative management.18 The incidence of a subsequent complication is highest in patients with severe disease on the initial CT scan.19
3. Contrast enema x-ray, cystography, ultrasound, and endoscopy are sometimes useful in the initial evaluation of a patient with suspected acute diverticulitis. Level of Evidence: III; Grade of Recommendation: B.
These other tests may be useful,20–25 especially if CT scan is not available. A gently administered single contrast enema x-ray may show stenosis/spasm with intact mucosa and associated surrounding diverticulosis. Strictures in diverticulitis are usually longer and more regular than in carcinoma. Fistulas and abscesses may be seen as well. Cystography is occasionally useful to confirm a colovesical fistula but may only demonstrate bladder wall thickening even if a fistula is present. Ultrasound of an inflammatory mass may help distinguish a phlegmon from an abscess,26 although overlying small bowel gaseous distension often obscures sonographic findings. Endoscopy has limited use in the acute setting and may exacerbate inflammation or cause perforation.27 Nevertheless, in selected cases with ambiguous features, a limited and gentle flexible sigmoidoscopy may be helpful in making an accurate diagnosis.
Medical Treatment of Acute Diverticulitis
For the purposes of this discussion, complicated diverticulitis is defined as acute diverticulitis accompanied by abscess, fistula, obstruction, or free intraabdominal perforation.
1. Nonoperative treatment typically includes dietary modification and oral or intravenous antibiotics. Level of Evidence: III; Grade of Recommendation: B.
Conservative treatment of acute uncomplicated diverticulitis is successful in 70 to 100 percent of patients.10,15,16,28–33 Uncomplicated diverticulitis may be managed as an outpatient (dietary modification and oral antibiotics) for those without appreciable fever, excessive vomiting, or marked peritonitis, as long as there is the opportunity for follow-up. The patient should be able to take liquids and antibiotics by mouth. Hospitalization for treatment (dietary modification and intravenous antibiotics) is usually best if the above conditions are not met, or if the patient fails to improve with outpatient therapy. Antibiotics should be selected to treat the most common bacteria found in the colon: gram-negative rods and anaerobic bacteria.13 Single and multiple antibiotic regimens are equally effective, as long as both groups of organisms are covered.30 Nonoperative treatment will resolve acute diverticulitis in 85 per-cent of patients, but approximately one-third will have a recurrent attack,11,12,18 often within one year. Long-term fiber supplementation after recovery from a first episode of diverticulitis may prevent recurrence in >70 percent of patients followed for more than five years.34,35 The likelihood of death from uncomplicated diverticulitis treated medically is low.36 Immunosuppressed or immunocompromised patients with acute diverticulitis are more likely to present with perforation or fail medical management.11,13,37
2. Radiologically guided percutaneous drainage is usually the most appropriate treatment for patients with a large diverticular abscess. Level of Evidence: III; Grade of Recommendation: B.
Approximately 15 percent of patients with acute diverticulitis will develop a pericolonic or intramesenteric abscess.38,39 For these patients, hospitalization and intravenous antibiotics are indicated. Abscesses <2 cm in diameter may resolve without further intervention. Patients with larger abscesses are candidates for percutaneous catheter drainage; the majority of patients can avoid an emergency operation and a multistaged approach involving a stoma by using this intervention.11,39,40
Evaluation After Recovery From Acute Diverticulitis
1. After resolution of an initial episode of acute diverticulitis, the colon should be adequately evaluated to confirm the diagnosis. Level of Evidence: V; Grade of Recommendation: D.
Colonoscopy or contrast enema x-ray (probably with flexible sigmoidoscopy) is appropriate to exclude other diagnoses, primarily cancer, ischemia, and inflammatory bowel disease.
Emergency Surgery for Acute Diverticulitis
1. Urgent sigmoid colectomy is required for patients with diffuse peritonitis or for those who fail nonoperative management of acute diverticulitis. Level of Evidence: III; Grade of Recommendation: B.
If a patient presents with severe or diffuse peritonitis, emergency colon resection is necessary. Also, if sepsis does not improve with inpatient conservative treatment of acute diverticulitis or after percutaneous drainage, surgery is indicated. Immunosuppressed or immunocompromised patients are more likely to present with perforation or fail medical management,11,12,37 so a lower threshold for urgent or elective surgery should apply to them. After emergency sigmoid resection, anastomosis might be performed, depending on the status of the patient and the severity of intra-abdominal contamination (Hinchey classification). A traditional Hartmann procedure is commonly performed (sigmoid colectomy, end sigmoid or descending colostomy, and closure of the rectal stump); however, the later second-stage operation to close this colostomy can be technically difficult. Furthermore, such temporary colostomies often are never closed.40 Alternatives to a Hartmann procedure may be primary anastomosis with or without intraoperative colonic lavage,41 or resection and anastomosis with temporary diverting ile-ostomy.42 The precise role and relative safety of primary anastomosis, especially without proximal diversion remains unsettled.43–45
Elective Surgery for Acute Diverticulitis
1. The decision to recommend elective sigmoid colectomy after recovery from acute diverticulitis should be made on a case-by-case basis. Level of Evidence: III; Grade of Recommendation: B.
After successful medical treatment of an episode of acute diverticulitis, careful judgment is required concerning whether to proceed with subsequent elective colon resection. After one attack, about a third of patients will have a later second attack of acute diverticulitis, and after a second episode, a further third will have yet another attack.10,11 The decision to recommend surgery should be influenced by the age and medical condition of the patient, the frequency and severity of the attack(s), and whether there are persistent symptoms after the acute episode. Most patients who present with complicated diverticulitis do so at the time of their first attack, therefore, a policy of elective colon resection after recovery from uncomplicated acute diverticulitis might not decrease the likelihood of later emergency surgery or overall mortality.10,36,37,46,47 Therefore, the number of attacks of uncomplicated diverticulitis is not necessarily an overriding factor in defining the appropriateness of surgery. As noted earlier, CT graded severity of a first attack is a predictor of an adverse natural history and may be helpful in determining the need for surgery.18 Inability to exclude carcinoma is another appropriate indication for colectomy.
There is no clear consensus regarding whether younger patients (younger than aged 50 years) treated for diverticulitis are at increased risk of complications or recurrent attacks.1,10–12,47 Nevertheless, because of their longer life span, younger patients will have a higher cumulative risk for recurrent diverticulitis, even if the virulence of their disease is no different than that of older patients.
2. Elective colon resection should typically be advised if an episode of complicated diverticulitis is treated nonoperatively. Level of Evidence: III; Grade of Recommendation: B.
After percutaneous drainage of a diverticular abscess, a later colectomy usually should be planned, because 41 percent of patients will otherwise develop severe recurrent sepsis.48 The safety of expectant management alone in this scenario remains suspect, although nonoperative management has been suggested.49
3. The resection should be carried proximally to compliant bowel and extend distally to the upper rectum. Level of Evidence: III; Grade of Recommendation: B.
It is usually sufficient to remove only the most severely affected segment; however, the proximal margin of resection should be in an area of pliable colon without hypertrophy or inflammation. Not all of the diverticulabearing colon must be removed. Usually a sigmoid colectomy will suffice; however, occasionally the proximal resection margin must extend well into the descending colon or to the left transverse colon. Distally, the margin of resection should be where the taenia coli splay out onto the upper rectum. After sigmoid colectomy for diverticulitis, an important predictor of recurrent diverticulitis is a colosigmoid rather than a colorectal anastomosis.12,50
4. When a colectomy for diverticular disease is performed, a laparoscopic approach is appropriate in selected patients. Level of Evidence: III; Grade of Recommendation: A.
Laparoscopic colectomy may have advantages over open laparotomy, including less pain, smaller scar, and shorter recovery. There is no increase in early or late complications.51,52 Cost and outcome are comparable to open resection.53 Laparoscopic surgery is acceptable in the elderly54 and seems to be safe in selected patients with complicated disease.55